|
Guidelines at Diagnosis | About Clinical Trials |
|
|
evidence-based support and information |
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Rituxan: Full prescribing information Rituxan.com |
|
Rituxan: ChemIDplus.gov
|
|
Rituxan overview www.omsusa.org | Medlineplus |
|
Rituxan: Dosage and Administration Guide Rituxan.com |
|
From the bench to the bedside: ways to improve rituximab efficacy (technical) bloodjournal.org PDF
|
Contact the company (now Biogen IDEC) idecpharm.com |
|
Off-Label Uses of Monoclonal Antibodies for Treatment of
|
|
Rituxan in Canada? cancercare.on.ca |
|
Rituxan - Help for patients who are underinsured or uninsured NeedyMeds
|
Unique Toxicities and Resistance Mechanisms Associated with Monoclonal Antibody Therapy
|
|
Optimal Schedule of Antibodies: Rituximab in Lymphoma as an Example,
|
|
Rituximab therapy for follicular lymphoma: a comprehensive review of it's efficacy as
|
|
Monoclonal Antibody Therapy for Non-Hodgkin's Lymphoma
|
|
Rituximab anti-CD20 antibody therapy of B cell non-Hodgkin's lymphomas - David C. Maloney Haematologica 1999. PDF |
|
Rituxan in Perspective - includes abstract, timeline, and more Rituxan.com |
Rituxan® (Rituximab) is indicated for ( www.rituxan.com/lymphoma/HCP/index.jsp ) Jan 2007
|
The treatment of patients with relapsed or refractory, low-grade or follicular, CD20-positive, B-cell, non-Hodgkin's lymphoma. |
|
|
The first-line treatment of diffuse large B-cell, CD20-positive, non-Hodgkin's lymphoma in combination with CHOP or other anthracycline-based chemotherapy regimens. |
|
|
The first-line treatment of follicular, CD20-positive, B-cell non-Hodgkin’s lymphoma in combination with CVP chemotherapy. |
|
|
The treatment of low-grade, CD20-positive, B-cell non-Hodgkin's lymphoma in patients with stable disease or who achieve a partial or complete response following first-line treatment with CVP chemotherapy. |
See Indications below
Rituxan in Canada? cancercare.on.ca
This is a commonly asked question and we believe the answer is yes, that adding Rituxan to the chemo is generally recommended even if you haven't responded well to prior Rituxan monotherapy.
While Rituxan alone might not be enough to tilt the balance of survival forces (die vs. don't die signals) within a cell to favor apoptosis*, it could well be sufficient to sensitize the lymphoma cells to the effects of chemotherapy.
* Apoptosis protects the body by getting rid of defective cells. It is a kind of suicide program that is carried out by the cell when defects are detected within the cell. (Peeling skin cells in reaction to sun burn is a common example).
… Lymphoma cells are thought to have defects in the apoptosis program. Both Rituxan and chemo are thought to be active against lymphoma cells by activating the self-destruct program -- chemo by damaging the dividing cells further; Rituxan by altering the pro-survival signals within the cells in a way that favors self-destruction.
Rituxan has other immune-mediated mechanisms of action, which may be strong or weak depending on normal variations in characteristics of the immune system. These mechanisms may not be as important when Rituxan is combined with chemotherapy (which depresses immunity).
Most times a lack of responsiveness to Rituxan is not because the CD20 target no longer exists … loss of cd20 expression on lymphoma cells happens rarely. For example, responses to radioimmunotherapy (which depends on the cd20 target) are often very good in those who have Rituxan-resistant lymphoma.
In other words Rituxan and chemo are thought to be synergistic when combined.
Footnote: We should note that this notion of synergy hasn’t been tested in a controlled way in patients with lymphoma refractory to Rituxan monotherapy – to our knowledge. We suppose the decision to add Rituxan to chemo could depend also on how you define Rituxan-refractory, so conceptually it's also possible that leaving it out would not matter in many cases. Thus this seems to be an appropriate population to evaluate chemotherapy followed by vaccines - perhaps compared to Rituxan-based chemo.
Dose: "Many studies have been performed to optimize its dose and schedule, and more are ongoing. The dose of 375 mg/m2 has become standard, mainly because it shows activity and has little associated toxicity." 1
Interval between treatments and courses: "The half-life of rituximab is about 1 week; median duration of persistence in the blood at active levels is of about 3 months: .... A prospective PK-based study by Gordan et al addressed the optimal interval between administrations. .... the great majority of patients could maintain active levels of drug with an infusion interval of 3 months, and all of the patients could be kept with blood levels in this range if they were treated every 2 months. We can therefore assume that an infusion of rituximab every 2–3 months should be sufficient to maintain tumors constantly exposed to active concentrations of the drug. This is actually the schedule that was chosen by many cooperative study groups for their maintenance strategy." 1
The goal of maintenance therapy is to "prolong the duration of chemotherapy-obtained remissions. "Data on long-term administration of rituximab are scarce and we need to await the results of prospective randomized trials of maintenance versus no maintenance before we can recommend this treatment as standard." 1
|
Type |
Dose | Infusions | Courses | Interval |
Study |
|
Standard (single agent) |
375 mg/m2 |
4 |
1 |
4x weekly |
JCO |
|
|
Approved by FDA at this schedule for relapsed NHL. The rationale based mostly on empiric and logistic considerations. 1 |
||||
|
Extended (single agent) |
375 mg/m2 |
8 |
1 |
4 x weekly |
AO |
|
|
Rationale: "The pharmacokinetic (PK) analysis in the first pivotal study of rituximab indicated that patients maintaining a higher and more prolonged blood level of rituximab had an increased chance of responding" 1 |
||||
|
Scheduled Retreatment (single agent) |
375 mg/m2 |
4 |
4 |
4 x weekly, |
JCO |
|
|
Patients restaged at week 6 for response; those with objective response or stable disease received maintenance rituximab courses (identical dose and schedule) at 6-month intervals |
||||
|
Scheduled retreatment |
375 mg/m2 |
4 |
variable |
4 x weekly VS. Scheduled: 1 X |
NCT00075946 |
|
|
Comparing scheduled vs rituximab retreatment for patients who respond (PR/CR) to standard dose of Rituxan. |
||||
|
Maintenance (after chemo) |
375 mg/m2 |
1 |
variable |
1 x at 8 week intervals for 1 to 2 years |
MAXIMA |
|
|
MAXIMA study objective is to evaluate the safety and efficacy of MabThera (Rituxan) maintenance therapy following a MabThera-containing induction regimen in first line or relapsed patients with follicular non-Hodgkin's lymphoma. |
||||
|
Maintenance (after chemo) |
375 mg/m2 |
1 |
~12 |
1 x at 8 week intervals for 2 years. |
PRIMA |
|
|
First period: Induction of response with 8 x rituximab, 375 mg/m2/dose |
||||
|
Consolidation post-ASCT |
375 mg/m2 |
4 |
1 |
4 x weekly, |
AO |
|
|
"One single course of rituximab after ASCT is safe, may help to eliminate MRD and may translate into improved EFS in both FL and MCL patients." See AO |
||||
.
Click to enlarge | Source rheuma-online.de
CD20 is GOOD TARGET for b-cell lymphomas (notes from 2007 presentation by Dr. Maloney)
- Not tumor specific, but b cell restricted
- Not custom made - off the shelf
- Has minimal hematologic or other toxicity other than infusion-related symptoms
- High expression level in most histologies (subtypes), except low level on most CLL
- Present on all tumor cells
- Infrequently lost in progression
But CD20 target is not an IDEAL target:
- Causes b-cell depletion (but does not effect immature b-cells)
- Does not have critical biologic function for survival of malignant cells
- CD20 negative b cell NHL's do occur, but rarely
- Selective pressure could lead to escape mutations
- Has only modest direct effects"Anti-CD20 therapy has had a truly dramatic impact on treatment and outcome of patients with follicular lymphoma. Unfortunately, the majority of responses to single-agent rituximab are incomplete, and all patients with follicular lymphoma will experience disease progression at some point following rituximab therapy.
Rituximab has multiple mechanisms of inducing in vivo cytotoxicity, including antibody-dependent cell-mediated cytotoxicity (ADCC), complement-dependent cytotoxicity (CDCC), direct apoptotic signaling, and possible vaccinal effects. Rituxan also increases the sensitivity of lymphoma cells to several chemotherapy agents.
The cellular microenvironment within follicular lymphoma has a profound impact on which mechanism is dominant, and confers resistance in many situations. Both tumor-associated and host-associated factors also contribute to rituximab resistance."- Unique Toxicities and Resistance Mechanisms Associated with Monoclonal Antibody Therapy, Jonathan W. Friedberg See asheducationbook.org
Rituxan is genetically engineered from portions of mouse and human antibodies and is produced through recombinant DNA technology.
| Review and print out the Dosage and Administration Guide for details Rituxan.com This will help familiarize yourself with the details of the procedure and allow you to ask informed questions. |
|
| Do not be shy about asking questions of your doctor about your specific risk factors in advance of the treatment. (... " pre-existing cardiac and pulmonary conditions, those with prior clinically significant cardiopulmonary adverse events, and those with high numbers of circulating malignant cells ( |
|
| You should plan to stay the day for the first infusion -- which should be given very slowly to minimize infusion-related risks. If you tolerate the first infusion well, you may be done in as little as three hours after that. |
|
| Prepare a thank-you-in-advance gift, such as baked goods, for the nursing staff. They work very hard and appreciate being appreciated. |
|
| Arrange to have a friend or relative accompany you, if at all possible. The therapy can make you drowsy and impact your ability to drive. |
|
| Bring your favorite reading material, or a portable audiotape/CD player with headphones to help pass the time. |
|
| Bring some favorite snacks, bottled water, and a pillow as well. Many centers will have snacks and drink available. |
|
| Be positive! Most patients have little problem at all. It's common to experience fatigue for the remainder of the day, and the next day as well. |
Monitoring your reactions
| Talk to the nurse and your doctor about treatment risks and what they will do to monitor you. Indicate that you are in no hurry to complete the infusion and that you will appreciate being monitored closely, especially the first time. |
|
| Ask the nurse or doctor about sensations that are to be expected and what to report immediately. Also refer to the Dosage and Administration Guide for details. |
|
| Just before treatment, you will also receive Tylenol in pill form. |
|
| You will receive Benadryl to help you tolerate the infusion better. This will make you drowsy. The same IV used to administer the Benadryl will be used to administer the Rituxan. The Benadryl may cause a temporary burning sensation. |
|
| The rate of administering the Rituxan is very slow at the start; it may be increased when it's determined you are tolerating it well. |
|
| Your vitals (temperature and blood pressure) will be taken and monitored throughout the treatment session, as often as every 30 minutes. Use this time to report unusual sensations. |
|
| Notify the nurse when you have any unusual sensations. |
The above Rituxan checklist - Print version
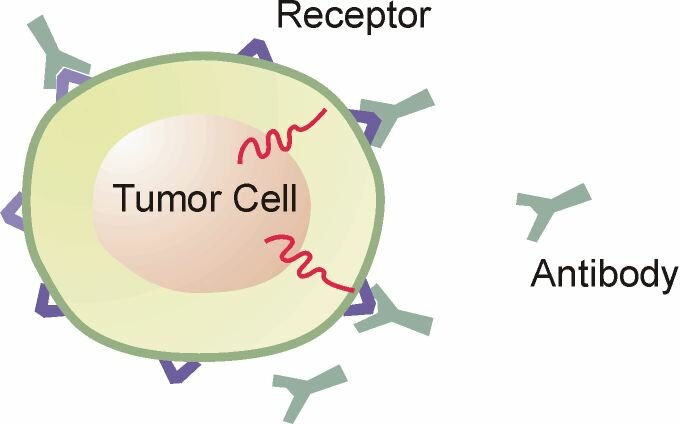
Rituxan circulates in the lymphatic system and tissue. It binds specifically to the CD20 antigen, a molecule present on the surface of the normal and malignant pre-B and mature B cells. This binding can be imagined as a lock fitting a key. More than 90 percent of B-cell NHL express CD20. Once bound to B-cells, Rituxan induces lysis (destruction of the cell) through several possible mechanisms:
| Apoptosis: The Rituxan antibody induces cells to which it is bound to initiate programmed cell death. The activation of this program by the cell results in the death of the cell (a kind of suicide). |
|
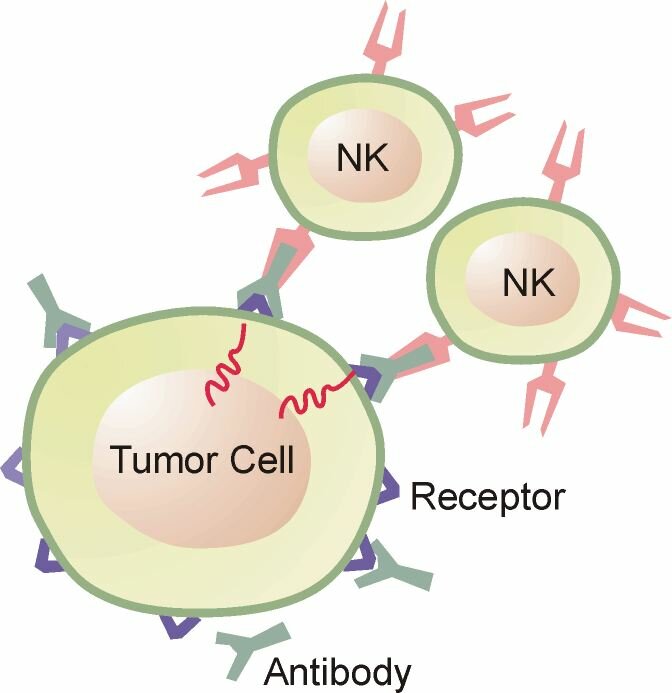
| Antibody-dependent Cell-mediated Cytotoxicity (ADCC) - An immune response triggered by the presence of antibody coating the target cell. Upon binding its antigen, the Antibody's Fc region is exposed and will bind its receptor on the NK cell (or other effector cells) to form a bridge. Once the bridge is formed, a poorly understood lytic (killing) signal is delivered to the target cell by the effector cell, resulting in its demise. |

Click image to enlarge.
| Complement-dependent cytotoxicity (CDC): A mechanism in which antibody bound to the target cell surface fixes complement, which results in assembly of the membrane attack complex that punches holes in the target cell membrane resulting in subsequent cell lysis. Dr David J. Flavell |
|||
| Inhibition of proliferation: The Rituxan antibody sends signals to the cell that stops the cell from dividing further. |
|||
| Vaccinal effect - when a therapy leads to recognition of tumor antigens (abnormal proteins) as foreign leading to an attack of the remaining tumors by effector cells in the immune system. |
|||
Synergistic effects with chemotherapy: The Rituxan antibody sends signals to the cell that sensitizes it to killing mechanisms of chemotherapy agents. Shifts it towards apoptosis, perhaps.
|
| Semin Hematol - Weiner: Rituximab: mechanism of action snip on challenges for discovery: "the conditions we have available in the research laboratory vary significantly from the real-world clinical environment. Studies of rituximab mechanisms of action often utilize rapidly dividing tumor lines that have been selected based on their ability to grow rapidly in vitro, and sometimes their relative sensitivity to therapy. Effector cells, when present, are usually not syngeneic and often come from normal donors, not patients with malignancy. In vivo, lymphocyte behavior changes within seconds of cells being exposed to hypoxic conditions (6). It takes minutes to hours to harvest, wash and otherwise manipulate peripheral blood cells for in vitro analysis." |
|
| AACR - Czuczman: Acquirement of Rituximab Resistance in Lymphoma Cell Lines Is Associated with Both Global CD20 Gene and Protein Down-Regulation Regulated at the Pretranscriptional and Posttranscriptional Levels snip: "It is postulated that the majority of patients retreated with rituximab will eventually relapse with variable degrees of resistant disease (16). There is an urgent need to conduct translational studies that will explore the mechanisms of resistance to mAbs in non–Hodgkin's lymphoma (NHL), and to develop therapeutic strategies to limit and/or overcome resistance pathways." |
|
| Blood - Hilchey: Rituximab immunotherapy results in the induction of a lymphoma idiotype-specific T-cell response in patients with follicular lymphoma: support for a “vaccinal effect” of rituximab "Given that the Id-specific responses shown in this study were not very robust, to elicit such clinically relevant responses, rituximab treatment will need to be coupled with strategies designed to overcome the FL-induced inhibition of the immune response." |
Types | Common | Incidence of | Serious infusion-related | Other Risks: Rare, Viral, Immune deficiency
|
TYPES:
|
COMMON:
|
"Incidence of Side Effects (Adverse Events) in > 5% of Patients with Relapsed or Refractory, Low-Grade or Follicular NHL, Receiving Single-agent Rituxan (N=356)a,b
See also eHealthMe.com reports
NOTE: AE rates in this one study (non-random sample; probably younger patients)
may not predict the incidence of AEs in the general population (of patients who use Rituxan to treat disease).
See also Grades of Toxicity
|
TYPE |
All Grades (%) |
Grade 3 and 4 (%) |
|
Any Adverse Events |
99% |
57% |
|
Body as a Whole |
86% |
10% |
|
Fever |
53% |
1% |
|
Chills |
33% |
3% |
|
Infection * |
31% |
4% |
|
Asthenia |
26% |
1% |
|
Headache |
19% |
1% |
|
Abdominal Pain |
14% |
1% |
|
Pain |
12% |
1% |
|
Back Pain |
10% |
1% |
|
Throat Irritation |
9% |
0 |
|
Flushing |
5% |
0 |
|
Cardiovascular |
25% |
3% |
|
Hypotension (low blood pressure) |
10% |
1% |
|
Hypertension (high blood pressure) |
6% |
1% |
|
Digestive |
37% |
2% |
|
Nausea |
23% |
1% |
|
Diarrhea |
10% |
1% |
|
Vomiting |
10% |
1% |
|
Hemic and Lymphatic System |
67% |
48% |
|
Lymphopenia |
48% |
40% |
|
Leukopenia |
14% |
4% |
|
Neutropenia |
14% |
6% |
|
Thrombocytopenia (low platelets) |
12% |
2% |
|
Anemia |
8% |
3% |
|
Metabolic and Nutritional Disorders |
38% |
3% |
|
Angioedema |
11% |
1% |
|
Hyperglycemia (high blood sugar) |
9% |
1% |
|
Peripheral Edema (swelling of tissues) |
8% |
0 |
|
LDH Increase (blood test marker) |
7% |
0 |
|
Musculoskeletal System |
26% |
3% |
|
Myalgia (muscle pain) |
10% |
1% |
|
Arthralgia (pain in the joints) |
10% |
1% |
|
Nervous System |
32% |
1% |
|
Dizziness |
10% |
1% |
|
Anxiety |
5% |
1% |
|
Respiratory System |
38% |
4% |
|
Increased Cough |
13% |
1% |
|
Rhinitis (irritation and |
12% |
1% |
|
Bronchospasm (difficulty in breathing |
8% |
1% |
|
Dyspnea (shortness of breath) |
7% |
1% |
|
Sinusitis |
6% |
0% |
|
Skin and Appendages |
44% |
2% |
|
Night Sweats |
15% |
1% |
|
Rash |
15% |
1% |
|
Pruritus (itching) |
14% |
1% |
|
Urticaria |
8% |
1% |
Adapted from: Full Prescribing Information gene.com
* Infection when Rituxan is used as monotherapy:
"There were sustained reductions in serum levels of both IgM and IgG observed from 5 through 11 months following single agent RITUXAN administration, which were statistically significant. It is important to note that only 14% of patients had reductions in serum IgM and/ or IgG to values below the normal range.1 Despite profound B-cell depletion, the incidence of infection did not appear to be increased. During treatment in the large multicenter trial of single-agent RITUXAN, 68 infectious events occurred. Of these, 7 were Grade 3 and none were Grade 4.5" http://www.rituxan.com/lymphoma/HCP/Files/PDFs/HCP_Q&A_Guide.pdf
Because of its specificity of action (it targets specific cells), Rituxan is generally less toxic than chemotherapies. However, it's not uncommon for patients to experience transient side effects -- mainly mild to moderate flu-like symptoms (fever, chills, rigors).
However, some patients may experience significant side effects. Most commonly, these adverse events occur during the first infusion. Severe and fatal reactions are uncommon but have occurred. See box warning below.
About Infusion-related reactions:
|
|
About HAMA PAL |
|
Some patients taking Rituxan may experience bowel obstruction aol.mediresource.com
|
|
Box warning for possible severe side effects IDEC
|
|
Serum sickness (uncommon) : "shivering fever (38.5°C) and polyarthralgias presented.
|
|
Tumor lysis syndrome (uncommon) : "Rituximab-induced ATLS has been reported in
|
Results. Severe hypersensitivity reactions are rare, with an incidence of
5%, provided patients receive proper premedication, close monitoring, and prompt intervention when symptoms occur.
Reactions to taxanes and monoclonal antibodies produce similar symptoms, but are generally immediate, occurring during the first few minutes of the first or second infusion. However, 10%–30% of reactions to monoclonal antibodies are delayed, and may occur in later infusions, indicating the importance of close observation of the patient following administration.
Mild-to-moderate reactions can be managed by temporary infusion interruption, reduction of the infusion rate, and symptom management. Rechallenge should be considered after complete resolution of all symptoms.
Severe reactions may require treatment discontinuation.
Conclusion. Hypersensitivity or infusion reactions to platinum compounds are acquired; reactions to taxanes and monoclonal antibodies are immediate and typically occur during the first few minutes of the first infusion. The different time of onset should be considered when developing strategies for preventing and managing hypersensitivity reactions. The decision to rechallenge or discontinue treatment after a reaction occurs depends on the severity of the reaction and other clinical factors.
Clinical applications of drug desensitization in the Asia-Pacific region http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3206230/ |
"Principles in drug desensitization
Several cardinal principles in drug desensitization [4, 5, 27] for drug allergy/hypersensitivity are as follows:
• There is no alternative drug available for the treatment of the underlying condition (e.g. allopurinol in chronic tophaceous gout, penicillin in pregnant women with syphilis, platinum salts in recurrent ovarian cancer).
• The drugs for the treatment of the underlying condition are superior to the alternatives (e.g. isoniazid for tuberculosis).
• The initial reaction should not be potentially life-threatening reaction. Drug induced hypersensitivity syndrome (DiHS), Stevens Johnson syndrome (SJS), toxic epidermal necrolysis (TEN) are absolute contraindications to desensitization. However, anaphylaxis is not a contraindication.
• The benefits of desensitization outweigh the risks of recurrence of drug hypersensitivity/allergy.
• Starting doses are at 1:1,000,000 to 1:100 of the target therapeutic dose depending on the severity of the initial reaction, or based on end-point intradermal skin testing to a non-irritative concentration of the drug.
• Dose escalations are doubled at 15-30 min intervals for immediate reactions, or at intervals of up to 24 h for non-immediate reactions.
• Close monitoring and resuscitative equipment with staff trained in resuscitation should be available for rapid desensitization.
• Pre-medications with systemic corticosteroids or anti-histamines should be avoided.
• Concomitant medical conditions should be stable (e.g. asthma, cardiac insufficiency).
• The patient is still deemed allergic to the drug to which he/she has been successfully desensitized.
• The patient must adhere to the drug daily in order for tolerance to be maintained, unless breakthrough reactions occur where dose escalations may need to be interrupted/slowed down.
• In desensitization for non-immediate reactions, periodic monitoring of complete blood count and liver enzymes should be considered prior to interval dose escalations.
|
J Allergy Clin Immunol. 2008 Hypersensitivity reactions to chemotherapy: outcomes and safety of rapid desensitization in 413 cases. http://www.ncbi.nlm.nih.gov/pubmed/18502492Ninety-eight patients who had HSRs in response to treatment with ... or rituximab received rapid desensitization to these agents. A standardized 12-step protocol was used, with treatment given intravenously or intraperitoneally. Initial desensitizations occurred in the medical intensive care unit, whereas most subsequent infusions took place in an outpatient setting. Safety and efficacy of the protocol were assessed by review of treatment records. |
"Patients requiring close monitoring during first and all subsequent infusions include those with pre-existing cardiac and pulmonary conditions, those with prior clinically significant cardiopulmonary adverse events and those with high numbers of circulating malignant cells (> 25,000/mm3) with or without evidence of high tumor burden. IDEC
"Major risk factors include high numbers of circulating malignant lymphoma cells, pulmonary infiltrates or lymphoma involvement, and prior cardiovascular disease. This report updates the safety experience of Rituximab therapy with data from clinical trials and postmarketing safety experience, and examines how this information can be used to optimize therapy." See Optimizing the use of rituximab for treatment of B-cell non-Hodgkin's lymphoma: a benefit-risk update. Kunkel
Complement activation plays a key role in the side-effects of rituximab treatment.
|
Semin Hematol 47:187–198, 2010 Rituximab-Associated Infections
|
Monoclonal antibody-associated progressive multifocal leucoencephalopathy (PML)
|
|
Progressive multifocal leukoencephalopathy [PML] after Rituxan therapy in
|
|
"Hypoglycemia is a very rare toxicity of rituximab. The exact mechanism of rituximab
|
Topic search: http://www.ncbi.nlm.nih.gov/
Inclusion of Rituximab in Treatment Protocols for Non-Hodgkin's Lymphomas and Risk for Progressive Multifocal Leukoencephalopathy http://1.usa.gov/1SC4oxv
|
|
Progressive multifocal leukoencephalopathy (PML) after rituximab therapy in
|
Late reactivation of resolved hepatitis B virus infection: an increasing complication post rituximab-based regimens treatment? Am J Hematol. 2008 Aug;83(8):673-5. PMID: 18528824 |
|
Rituximab-related viral infections in lymphoma patients.
|
|
Hepatitis B virus reactivation in a case of non-Hodgkin's lymphoma treated with
|
|
Shingles reactivation? One case reported on nhl-follic support list when
|
Topic Search: PubMed
Late Onset Neutropenia:
2011, Expert Review: Late-onset neutropenia following rituximab therapy: incidence, clinical features and possible mechanisms, Daniel Tesfa* and Jan Palmblad
Late-onset neutropenia (LON) is emerging as a common adverse effect to rituximab therapy owing to widespread use of this drug in the treatment of B-cell lymphomas and autoimmune diseases. However, the true incidence and mechanisms are not fully understood.
LON has been reported in 5–27% of rituximab-treated lymphoma patients. Similar figures apply for autoimmune patients but they appear to have more infections during the neutropenic period.
Recent reports imply that host factors may play an intriguing role for development of LON, for example, polymorphisms in FCGR3.
Pronounced B-lymphocyte depletion and lower serum IgM, as reported in LON patients during the period of neutropenia compared with matched controls, may play a role for understanding the mechanisms and risk stratification for emergence of LON. expert-reviews.com
Rituxan and late onset neutropenia following Auto stem cell transplants haematologica.org |
|||
Rituxan and Late-onset neutropenia (LON) ncbi.nlm.nih.gov
|
Serum sickness"Serum sickness is a reaction similar to an allergy. Specifically, it is an immune system reaction to certain medications, injected proteins used to treat immune conditions, or antiserum, the liquid part of blood that contains antibodies that help protect against infectious or poisonous substances." MedlinePlus.gov |
|
Effect of prior rituximab on high-dose therapy and autologous stem cell transplantation in follicular lymphoma. Bone Marrow Transplant. 2007 Sep 17; PMID: 17873917
|
How long it takes for Rituxan to work can be very different from one person to the next. Rituxan works gradually, so don't' be discouraged if it takes a while to work for you. When Rituxan was tested, it often took several months after the completion of Rituxan treatment for the tumor to shrink.
Time to First Tumor Response in Efficacy Studies
Adapted from table in http://www.emea.europa.eu/humandocs/PDFs/EPAR/Mabthera/025998en6.pdf
Monotherapy
Studies (follicular NHL)Responders Average Time (Days) Median Time (Days) Min Time (Days) Max Time (Days) 102-02 -II
102-0517 of 37
80 of 16658.2
65.350
507
21112
288Total 97 of 203 64 50 7 288
The expected response rate is just an average (a statistic calculated for a large group) which cannot predict individual outcomes. Some factors that may influence individual outcomes are: treatment history, tumor burden, type of lymphoma, the number of infusions, serum levels that you obtain, other treatments you are receiving with Rituxan, and perhaps variable molecular characteristics of the malignant cells.
What is the expected time to initial response?
It can vary by lymphoma subtype. In one study in follicular lymphoma the median time to initial onset of response was 50 days. (Rituxan® full Prescribing Information, April 2001)
In a pivotal, multi-center study, Rituxan achieved an overall response rate of 48 percent (80/166.
Complete Responses (CR): Six percent (10/166) of patients had complete responses.
Partial Responses (PR): Forty-two percent (70/166) of patients.
Median Duration of Response: Projected to be 10 to 12 months.
Rituximab chimeric anti-CD20 monoclonal antibody therapy for relapsed indolent lymphoma: half of patients respond to a four-dose treatment program. J Clin Oncol. 1998 Aug;16(8):2825-33. PMID: 9704735 PubMed
Of interest is that median duration of responses can be longer than "the medians achieved in the patients' prior course of rituximab." This is not the rule for cancer treatments, and speaks to the potential of Rituxan and treatments with targeted mechanisms to better manage lymphomas.
Rituximab anti-CD20 monoclonal antibody therapy in non-Hodgkin's lymphoma: safety and efficacy of re-treatment. J Clin Oncol. 2000 Sep;18(17):3135-43. PMID: 10963642 PubMed
Reports on factors associated with response to Rituxan
Absolute lymphocyte count (ALC) predicts therapeutic efficacy of rituximab therapy in follicular lymphomas. Br J Haematol. 2007 Apr 13 PMID: 17433025
This study supports our hypothesis that a higher ALC predicts longer TTP following rituximab therapy.Genetic characteristics (FCGR3A genotype) predict response to Rituxan? Blood 2002 Feb 1 | PubMed
Rituxan review article Medscape (free login req.)
CLL/SLL: Rituximab using a thrice weekly dosing schedule in B-cell chronic lymphocytic leukemia and small lymphocytic lymphoma demonstrates clinical activity and acceptable toxicity. J Clin Oncol. 2001 Apr 15;19(8):2153-64. PMID: 11304767 PubMed
Prognostic factors for non-Hodgkin's lymphoma patients treated with chemotherapy
may not predict outcome in patients treated with rituximab.
Leuk Lymphoma. 2006 Sep;47(9):1830-40 PMID: 17064996Serum levels of Rituxan may influence efficacy Berinstein
Extended Rituximab (anti-CD20 monoclonal antibody) therapy for relapsed or refractory low-grade or follicular non-Hodgkin's lymphoma. PubMed abstract
Rituxan as frontline treatment "With further follow-up and repeat courses of rituximab, the major response rate increased from 47% to 65% and the complete response rate increased from 7% to 27%."
Semin Oncol 2002 Feb;29(1 Suppl 2):25-9 abstract 4-09-02
![]() TOPIC SEARCH PubMed
TOPIC SEARCH PubMed
Rituxan kills both normal and malignant b-cells that express CD20. Precursor cells from which new b-cells are generated do not express CD20 and are not affected. B-cell recovery begins at approximately six months following completion of treatment, and median B-cell levels return to normal by 12 months.
B cell reconstitution after rituximab treatment of lymphoma recapitulates B cell ontogeny.Clin Immunol. 2007 Feb;122(2):139-45. Epub 2006 Sep 27 PMID: 17008130
|
|
Immunophenotypic changes and clinical outcome in B-cell lymphomas treated with rituximab.
|
Association between rituximab use and progressive multifocal leukoencephalopathy (PML) among non-HIV, non-Hodgkin lymphoma Veteran’s Administration patients. | 2014 ASCO Annual Meeting Abstracts http://bit.ly/1t7c3qY |
|
News medical: MCCIR scientists use video imaging to investigate
|