|
Guidelines at Diagnosis | About Clinical Trials |
|
|
evidence-based support and information |
|
|
|
|
Efficacy of RIT - Related citations
Clinical considerations and risks of RIT - an overview There is no avoiding risk. When we make a decision we trade one kind of risk for another. Virtually all approaches to managing lymphoma will have risks, including observation. Chemotherapy-based protocols also have risks, some of these are similar to RIT. What follows are some generally accepted principles that can help patients to make an informed choice in consultation with their physicians. Risk/benefit assessments: We can think of induction therapies as approaches to treatment having greater possible risks but also having greater potential reward. The intent or goal of induction therapy is to achieve a more durable remission and possible cure. Using this definition, both RIT and Rituxan-based chemotherapy are induction approaches - having different types of risks, durations on treatment, and side effects. Apples to Oranges: it's challenging to compare the possible risks and potential benefits of RIT with chemotherapy approaches. The same holds for comparing Rituxan (a management approach) to RIT (an induction therapy). An induction treatment having more possible side effects or more significant but uncommon serious risks, may have less risk overall when or if it achieves a durable remission ... compared to management with a drug with lower toxicity given repeatedly over many years. Treatment history: The best opportunity to achieve a durable remission from standard treatments is with initial therapy and first or second relapse. Tumor burden and areas of presentation: The size of tumor can influence the potential for a durable response to treatment. For example, de-bulking treatment followed by consolidation with RIT might be considered if one or more tumors are very large. See also Bulky disease and RIT? Having high levels of lymphoma in the bone marrow or spleen can increase the risk of RIT because it emits radiation to bystander cells. See also: Relationship of degree of bone marrow involvement with hematologic toxicity in patients with non-Hodgkin's lymphoma treated with tositumomab and iodine I 131 tositumomab. ASCO 2003 Treatment-related MDS/AML (secondary cancers, which does not appear to be a greater for RIT than for chemotherapy) in patients with follicular lymphoma after frontline therapy with tositumomab and iodine I 131 tositumomab ASCO 2003
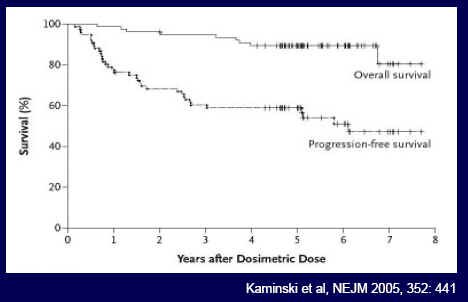
Harvesting Stem Cells for Transplant in Non-Hodgkin's Lymphoma Patients Is Still Possible After Treatment with Bexxar news.cornell.edu Competing choices: Recognition is needed that many patients when sufficiently informed about the unique properties of RIT may have a preference for RIT treatment over the competing choices. Being fully informed about all of our choices is not easy ... but should be standard practice. We urge the NCCN to develop patient materials for this purpose. Because of the dwindling usage of RIT, it's important to underline and communicate broadly about its unique positive properties: that RIT is the only potent (non-palliative), and tolerable induction therapy available to the elderly and frail. Fostering community access to RIT (by NRC policy decisions) is important because a good many people with lymphoma may be unable to travel to a nuclear medicine center due to their physical limitations. Further, people with limited income will not be able to afford the travel, or to take time off from work. Health insurance policies often restrict out-of-network use. As Einstein noted: "Not everything that counts can be counted." Clearly, an 8-fold increase in training will be a barrier to oncologists who might otherwise consider becoming authorized users of radioimmunotherapy. Oncologists who are not authorized to give RIT have an inherent conflict of interest -- it is a disincentive to inform patients about an approach to treating indolent lymphoma that they cannot administer. This is a major concern as it has been reported that 85% of cancer patients are treated in community setting - Cohen. Cancer J Clin 2003;53:73-81. Clinical trial results and its unique properties support the continued use and additional study of FDA-approved RIT. The durable outcomes that can be achieved with RIT (equivalent to chemotherapy) are rarely achieved with palliative measures (Rituxan, doublets, etc.). The outcomes were compelling in the Kaminski study of Bexxar for untreated follicular lymphoma. But the findings could not change practice because of the single-arm study design. NEJM, Kaminski, full text To date, we have not had a completed study comparing R-chemotherapy to RIT monotherapy, or RIT to Rituxan monotherapy. The lack of a definitive study on the superiority of RIT monotherapy likely contributes to the apparent incorrect perception among many oncologists that routinely informing patients about the unique properties of RIT is not required. Clinical impressions on the value of RIT in the relapse setting could well be from turning to this approach too late, when all approaches available to the community oncologist have been exhausted. Since not all patients with lymphoma can tolerate chemotherapy, it's vital that we utilize RIT fully when it's appropriate and/or preferred by the informed patient. The unique mechanistic properties of RIT provide a strong rationale for testing RIT give with targeted drugs and with other immunotherapies. Related articles
|
Zevalin Consolidation of First Remission in Advanced-Stage Follicular Non-Hodgkin Lymphoma: Median Follow-Up of 7.3 Years From the International, Randomized, Phase III First-Line Indolent Trial” http://bit.ly/1khWdEV
|
|
Br J Haematol 2013:
|
|
Zevalin - Medscape: Renewed Interest in Ibritumomab for NHL |
|
Zevalin, Fludarabine, and TBI-based "mini" allogeneic transplantation |
|
ASH Paper, 2013:
|
Who is Zevalin for?
Patients with relapsed or refractory low-grade, follicular, or transformed B-cell non-Hodgkin's lymphoma, including patients with Rituximab refractory follicular non-Hodgkin's lymphoma. Update: Zevalin is also indicated for the treatment of previously untreated follicular NHL in patients who achieve a partial or completed response to first-line chemotherapy.
Repeated Use of ZEVALIN? The entire ZEVALIN therapeutic regimen is intended as a one-time treatment. The safety profile from multiple courses of the ZEVALIN therapeutic regimen or other forms of therapeutic radiation preceding, following, or in combination with the ZEVALIN therapeutic regimen has not been established.
The effects of Zevalin on survival is unknown.
Mechanism of Action
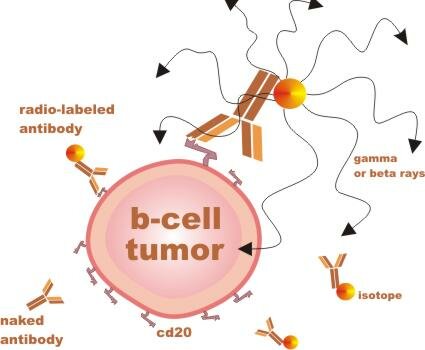
After Y-90 ZEVALIN (the therapeutic component of the ZEVALIN regimen) enters the bloodstream, the monoclonal antibody ibritumomab recognizes and attaches to the CD20 antigen, allowing beta radiation emitted by the Yttrium-90 isotope to penetrate and damage the B-cell as well as neighboring cells.
Treatment with ZEVALIN: The entire ZEVALIN therapeutic regimen is delivered over 7 to 9 days. Patients then receive follow-up care by a physician for at least an additional 12 weeks. The ZEVALIN therapeutic regimen can be administered entirely on an outpatient basis and no isolation or lead shielding is necessary.Where can I receive treatment?
You can use the Treatment Site Locator
How Zevalin Is Given?Note: The Bioscan step is no longer required with Zevalin therapy.
Zevalin is a two step protocol administered by IV over 7 to 9 days.
Step 1, Day 1: Rituxan infusion of 250 mg/m2 - starting at a slow rate.
Step 2: Seven to nine days later:
Rituxan infusion is given a second time as described above.
Within 4 hours the treatment dose of Zevalin (Zevalin linked with Yttrium-90)
is infused over 10 minutes.The dose of Zevalin given depends on many factors, including your height and weight, your general health or other health problems, and the type of cancer or condition being treated.
Ongoing Studies Clinical studies at major medical centers are currently investigating the use of the ZEVALIN therapeutic regimen in a variety of other lymphoma subtypes including aggressive disease. The ZEVALIN therapeutic regimen is also being studies in a number of different treatment strategies including combinations with front-line and salvage chemotherapy regimens and as part of autologous and allogeneic stem cell transplantation.
Contraindicated (not for): Patients with known Type I hypersensitivity or anaphylactic reactions to murine (mouse) proteins or to any component of this product, including Rituxan, yttrium chloride, and indium chloride. Zevalin should not be administered to patients with >25% lymphoma marrow involvement and/or impaired bone marrow reserve.
Median time to nadir (low blood counts): "Median time to ANC nadir was 62 days, to platelet nadir was 53 days, and to hemoglobin nadir was 68 days"
Source: Zevalin
Click to enlarge
Resources:
Zevalin Company Support, reimbursement and availability questions:
By Web: zevalin.com/
By Phone: 1-866-298-8433
Option 1: Customer Service / Orders
Option 2: Medical Information or Adverse Events Reporting
Option 3: Product Complaints
Option 4: Reimbursement
Option 5: Rituximab Questions
By Email:
Full prescribing information Zevalin.com
Does spleen involvement preclude use of radioimmunotherapy?
Splenectomy in Non-Hodgkin's lymphoma ncbi.nlm.nih.gov/books
Residual splenomegaly in a patient who has otherwise successfully responded in other sites following chemotherapy for lymphoma is another reason for performing a splenectomy. In these cases, the procedure may be performed for both diagnostic and therapeutic reasons; it can determine if the splenomegaly is due to persistent lymphoma, and should this be true, it can potentially eliminate the focus of residual disease. A less common indication for splenectomy that may be seen more frequently in the future is to allow patients to become eligible for enrollment onto novel treatment protocols. An example of this is in patients with lymphoma refractory to conventional chemotherapy who were treated with radioimmunotherapy using a radiolabelled anti-CD20 antibody.
In some of these patients, splenomegaly was found to complicate treatment, as the large organ served as an “antigen sink”, effectively decreasing the dose of radionuclide available to treat other sites of disease. Thus, pretreatment splenectomy may be indicated to eliminate this complicating factor.
Related Topics
Antibodies for NHL
|
ASH 2010: Zevalin-based abstracts
90Y-Ibritumomab Tiuxetan (Zevalin®) Consolidation of First Remission In Advanced-Stage Follicular Non-Hodgkin’s Lymphoma: Updated Results After a Median Follow-up of 66.2 Months From the International, Randomized, Phase III First-Line Indolent Trial (FIT) In 414 Patients http://ash.confex.com/ash/2010/webpr...aper28386.html SNIPS: The FIT trial was conducted to evaluate the safety and efficacy of 90Y-ibritumomab tiuxetan (0.4 mCi/kg; maximum dose 32 mCi) when used as consolidation of first complete or partial remission in patients with previously untreated, advanced-stage follicular lymphoma (FL). Patients were randomly assigned to either 90Y-ibritumomab treatment (n = 207) or observation (n = 202) within 3 months (mo) of completing initial induction therapy (chemotherapy only: 86%; rituximab in combination with chemotherapy: 14%). Results from the first extended follow-up after a median of 3.5 years revealed a significant improvement in PFS from the time of randomization with 90Y-ibritumomab consolidation compared with control (36.5 vs 13.3 mo, respectively; P < 0.0001; Morschhauser et al. JCO. 2008; Overall response rate to second-line treatment was 79% in the 90Y-ibritumomab group (57% CR/CRu and 22% PR) vs 78% in the control arm (59% CR/CRu, 19% PR). Five-year overall survival was not significantly different between the groups; 93% and 89% in the 90Y-ibritumomab and control groups, respectively (P = 0.561). To date, 40 patients have died; 18 in the 90Y-ibritumomab group and 22 in the control group. Secondary malignancies were diagnosed in 16 patients in the 90Y-ibritumomab arm vs 9 patients in the control arm (P = 0.19). There were 6 (3%) cases of myelodysplastic syndrome (MDS)/acute myelogenous leukemia (AML) in the 90Y-ibritumomab arm vs 1 MDS in the control arm (P = 0.063). Other Zevalin reports at ASH 2010: A Multi-Center Prospective Randomized Study Comparing Ibritumomab Tiuxetan (Zevalin) and High-Dose BEAM Chemotherapy (Z-BEAM) Vs. BEAM Alone as the Conditioning Regimen Prior to Autologous Stem-Cell Transplantation In Patients with Aggressive Lymphoma; Possible Advantage for Z-BEAM In Low-Risk Patients http://ash.confex.com/ash/2010/webpr...aper28200.html Phase II Study of 2-Weekly CHOP+Rituximab Followed by Yttrium-90 Ibritumomab Tiuxetan (Zevalin) In Patients with Previously Untreated Diffuse Large B Cell Lymphoma (DLBCL): Final Analysis http://ash.confex.com/ash/2010/webpr...aper27049.html The Risk of Secondary Myelodysplastic Syndrome/Acute Leukemia Following High-Dose Yttrium-90 Ibritumomab Tiuxetan Is Analogous to That Observed Following High-Dose Chemotherapy: a Matched-Pair Analysis In Non-Hodgkin Lymphoma Patients http://ash.confex.com/ash/2010/webpr...aper30605.html Update on a Prospective Study Evaluating the Safety and Efficacy of Combination Therapy with Fludarabine, Mitoxantrone and Rituximab Followed by Yttrium-90 Ibritumomab Tiuxetan and Maintenance Rituximab as Front Line Therapy for Patients with Indolent Lymphomas http://ash.confex.com/ash/2010/webpr...aper26924.html 90Yttrium Ibritumomab Tiuxetan as First Line Treatment for Follicular Lymphoma. First Results from an International Phase II Clinical Trial http://ash.confex.com/ash/2010/webpr...aper33702.html Bortezomib May Be Safely Combined with Y-90 Ibritumomab Tiuxetan In Patients with Relapsed/Refractory Follicular or Transformed Non-Hodgkin Lymphoma: A Phase I Trial of Combined Induction Therapy and Bortezomib Consolidation http://ash.confex.com/ash/2010/webpr...aper28666.html Comparative Analysis of Autologous Hematopoietic Cell Transplantation with Radioimmunotherapy (RIT) Based Conditioning Versus Total Body Irradiation (TBI) for High-Risk Diffuse Large Cell Lymphoma (DLCL): Toxicity and Efficacy http://ash.confex.com/ash/2010/webpr...aper29132.html 90Υ-Ibritumomab Tiuxetan Followed by Rituximab Is a Safe Treatment Option for Relapsed or Refractory Diffuse Large B-Cell Non-Hodgkin s Lymphoma http://ash.confex.com/ash/2010/webpr...aper31933.html |
Zevalin as a Single Agent in Patients With Pretreated B-Cell Lymphoma: Evaluation of the Long-Term Outcome http://bit.ly/doQm0a
|
|
NEW Radioimmunotherapy: FIT to be applied? Randomized study shows improved PFS by 2 yrs in follicular lymphoma when given as consolidation for chemotherapy Medscape.com ( login req.)
|
|
Zevalin Licensed For First Line Consolidation Therapy for fNH, May 2008 medicalnewstoday.com
|
|
Zevalin in Mantle Cell Lymphoma touchbriefings.com pdf 2007
|
|
Radiation dosimetry results and safety correlations from 90Y-ibritumomab tiuxetan radioimmunotherapy for relapsed or refractory non-Hodgkin's lymphoma: combined data from 4 clinical trials. J Nucl Med. 2003 Mar;44(3):465-74. PMID: 12621016
|
|
Salvage therapy for primary Central Nervous System lymphoma with (90)Y-Ibritumomab and Temozolomide. J Neurooncol. 2007 Jul;83(3):291-3. Epub 2007 Jan 24. PMID: 17245621
|
|
Zevalin: Risk of MDS/AML update www.fda.gov | Zevalin_PI.pdf
|
|
Analysis of the Incidence of Treatment-Related Myelodysplastic Syndrome and Acute Myelogenous Leukemia in Registration and Compassionate-Use Trials of Ibritumomab Tiuxetan Radioimmunotherapy (RIT). Session Type: Oral Session ASH 2006 |
|
Zevalin update: Biogen Idec and FDA notified healthcare professionals of revision to BOXED WARNINGS, WARNINGS, and ADVERSE REACTIONS sections of the Prescribing Information to describe severe cutaneous (skin) or mucocutaneous (mucosal linings) reactions, some with fatal outcome, that have been reported in association with the Zevalin therapeutic regimen in the post-marketing experience. fda.gov/medwatch | medpagetoday.com |
|
Follow-up results of a phase II study of ibritumomab tiuxetan radioimmunotherapy in patients with relapsed or refractory low-grade, follicular, or transformed B-cell non-Hodgkin's lymphoma and mild thrombocytopenia. Cancer Biother Radiopharm. 2004 Aug;19(4):478-81. PMID: 15453962 |
|
ASCO 2003 - Report on Zevalin - durable responses; safety as second- or third-line therapy Buswire |
|
4-year data: Safety of Yttrium-90 Ibritumomab Tiuxetan Radioimmunotherapy for Relapsed Low-Grade, Follicular, or Transformed Non-Hodgkin's Lymphoma. J Clin Oncol. 2003 Apr 1;21(7):1263-70. PMID: 12663713 PubMed |
|
Durable Remissions Obtained with Zevalin in Recurrent Follicular Lymphoma CancerConsultants.com |
|
Zevalin: Full Prescribing Information IDEC |
|
Subsequent Therapy Well Tolerated in Patients Previously Treated with Zevalin (tm) 411cancer.com |
|
Zevalin Reimbursement Support IDEC
|
|
Zevalin Safe For Patients Who Have Had Prior Radiation OncoLink 10-9-02 2002 (scroll down after reaching page) |
|
Subsequent Therapy Well Tolerated in Patients Previously Treated with Zevalin (tm) www.vacancer.com |
|
Biologic License Application PDF | PDF-Help |
|
90Y ibritumomab (Zevalin) in aggressive non-Hodgkin's lymphoma: analysis of response and toxicity Year: 2002 Abstract No: 1061 |
|
90Y ibritumomab tiuxetan (Zevalin) radioimmunotherapy does not preclude effective delivery of subsequent therapy for lymphoma Year: 2002 Abstract No: 1064 |
|
90Y-ibritumomab tiuxetan (Zevalin) radioimmunotherapy for transformed B-cell non-HodgkinÝs lymphoma (NHL) patients Year: 2002 Abstract No: 51 |
|
Randomized controlled trial of yttrium-90-labeled ibritumomab tiuxetan radioimmunotherapy versus rituximab immunotherapy for patients with relapsed or refractory low-grade, follicular, or transformed B-cell non-Hodgkin's lymphoma. J Clin Oncol. 2002 May 15;20(10):2453-63. PMID: 12011122 PubMed |
|
Ibritumomab tiuxetan radioimmunotherapy for patients with relapsed or refractory non-Hodgkin lymphoma and mild thrombocytopenia: a phase II multicenter trial. Blood. 2002 Jun 15;99(12):4336-4342. PMID: 12036859 PubMed (Lower dose used.) |
|
RIT and risk of MDS: Treatment-related myelodysplastic syndrome (MDS) and AML in patients treated with Zevalin radioimmunotherapy. J Clin Oncol. 2007 Sep 20;25(27):4285-92. Epub 2007 Aug 20.
|
 Introduction - About Zevalin:
Introduction - About Zevalin: